{kind=link}
In the follow-up to their article on the value of triage within mental health intervention in Occupational Health & Wellbeing last October, Dr William Badenhorst, Dr Lorenzo Grespi and Alison Garrow argue that interventions need to be anchored within a coherent framework.
In our previous article in Occupational Health & Wellbeing this time last year we suggested that triage can be a valuable method for dealing with mental health-related situations in the workplace – ensuring that any assessment or subsequent intervention is based on a clear rationale.
We emphasised, however, that this cannot take place in a vacuum and that the effective management of any mental health-related situations requires solid underpinning. This follow-up article describes the necessary framework required.
About the authors
Dr William Badenhorst is a consultant psychiatrist and deputy medical director of Grespi. Dr Lorenzo Grespi is a consultant psychiatrist and medical director of Grespi. Alison Garrow is a senior associate at workplace law firm Doyle Clayton
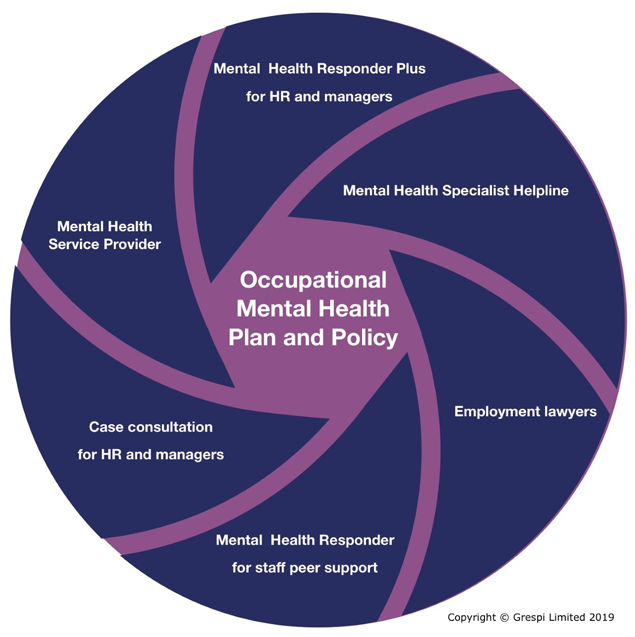
An effective approach to occupational mental health in an organisation is made up of a number of inter-related components that all need to work together coherently. The figure 1 image provides a visual representation of these components.
Central to this framework are two separate documents: the occupational mental health and wellbeing “plan” and the occupational mental health and wellbeing “policy”. We shall look at each in turn.
The occupational mental health and wellbeing plan
The plan is a strategic document that identifies priorities and appropriate actions to ensure that good mental health is promoted and mental ill health is addressed across the following three levels of intensity:
- The disclosed group. This is staff members whose mental health and wellbeing has already been disclosed as a problem.
- The high-risk group. This is staff members who are at higher risk of developing problems, primarily because of the nature of their work (such as high pressure, limited autonomy and so on) or their life circumstances (such as being recently bereaved or divorced, juggling significant care responsibilities outside work with unpredictable workload at work).
- The standard group. This is the remainder group of staff members whose mental health and wellbeing is not a high-risk problem but whose quality of life, loyalty and productivity might be improved by well-targeted mental health and wellbeing initiatives. Such initiatives might include enabling access to healthy food and exercise, ensuring a minimum work/life/sleep balance, organising constructive, inclusive work socials and so on.
The plan ensures the strategy is coherent, consists of clear objectives with implementation and review and is owned by the organisation’s senior leaders.
The occupational mental health and wellbeing policy
The policy is a document available to all employees and sets out the framework for how the occupational mental health and wellbeing plan translates into operational delivery.
It should make it clear which of the organisation’s other procedures and policies (such as health and safety, recruitment, disciplinary, anti-bullying and harassment policies) are linked to or affected by the plan.
The policy should demonstrate that the employer supports its employees’ mental health and wellbeing and affirm its commitment to provide a positive working environment. This is conducive to good mental health and goes a long way in addressing stigma or discrimination when employees suffer mental health problems.
The plan and policy are together dynamic documents, which form the foundation of the approach adopted by the employer towards mental health and inform continual revision and improvement.
The organisation should build supporting structures – both internal and external to the organisation, as again shown in figure 1.
Mental health responder plus programme (MHR Plus) and case consultations
MHR Plus is a training and backup programme designed for HR professionals and managers. It is aimed at enabling these key workplace professionals to deal effectively with the clinical, legal and organisational challenges posed by mental health-related situations in the workplace.
The programme adopts a modular format, with modules being combined as required, including:
- MHR Plus training;
- Digital platform updates;
- MHR Plus refresher courses;
- Balint Groups; and
- Case consultations.
MHR Plus training enables HR professionals and managers to communicate more effectively with employees experiencing psychological difficulties and mental health conditions.
It teaches them to observe, collect information and make initial formulations as a component part of the approach – “triage, assess, respond”. The training deals appropriately with psychological aspects of performance management and helps HR professionals remain in the driving seat on legal implications, including duty of care, confidentiality, disability discrimination, reasonable adjustments, and due diligence. It also provides guidance on the initial response to mental health emergencies.
MHR Plus-trained HR and managers should also rely on updates on mental health-related issues provided via digital platforms which should place an emphasis on practical advice on the handling of mental health situations at work. Digital platforms include email, Twitter and social media.
To ensure that the learning of MHR Plus-trained HR and managers continues evolving over time, it is recommended that MHR Plus-trained staff participate in MHR Plus refresher courses at regular six-monthly or annual intervals.
Support to HR and managers for complex mental cases should also take the form of case consultations provided on an ad hoc basis by occupational mental health specialists and organisational consultants as appropriate.
A further modular support option for HR and managers is provided through Balint Groups.
These are designed to help group members work more effectively in their role as HR managers via the discussion of problematic real-life workplace mental health-related situations.
Discussions also include the case-based review of established processes and procedures, organisational dynamics and outcome evaluation.
Balint Group sessions should be led by an occupational mental health specialist. They typically last for 75-minutes and are held monthly or fortnightly. Groups have a maximum of eight members who should preferably have completed the MHR Plus training.
Mental health specialist helpline
Ongoing support and advice to MHR Plus-trained HR and managers is provided by a mental health specialist helpline. The helpline should be staffed by senior occupational mental health specialists and provide telephone triage and advice to HR and managers on the management of mental health-related situations at work and of employees suffering from psychological and mental health problems.
The helpline is also the primary channel for referrals of employees requiring occupational mental health assessment; psychiatric and psychological assessment and treatment; therapies, including psychotherapy, CBT and counselling; occupational therapy in mental health; organisational consultancy; and wellbeing, including general counselling, mindfulness, yoga and Pilates.
Mental health service provider
The organisation’s mental health service provider is expected to address a range of mental health conditions of differing severity. A multi-disciplinary team made up of medical doctors/psychiatrists, psychologists, psychotherapists, counsellors and occupational therapists in mental health is best placed to provide effective and comprehensive clinical services.
The choice of treatment, discipline and clinician should primarily be determined by the employee’s clinical needs and provided by clinicians with the appropriate qualification, expertise and experience.
It is far preferable that the provider should be either medically-led or include the services of a named medical consultant psychiatrist in the capacity of medical director, even when the provider offers only counselling and psychotherapy services.
This is because the medical director has the duty to ensure all health services offered by a provider are in keeping with the guidelines of the General Medical Council (GMC), which represents the “gold standard” in healthcare. By adopting the GMC gold standard, both commissioning organisations and providers are on much firmer footing, for example when legal challenges are made on employers’ duty of care obligations and providers’ clinical governance expectations.
We would also like to stress that Employee Assistance Programmes (EAPs) should not be regarded or confused with specialist occupational mental health services, particularly when employees suffer from diagnosed mental health conditions – be it minor anxiety disorders or severe conditions like depressive episodes or Post-traumatic Stress Disorder (PTSD).
There is no doubt that EAPs have a role in providing psychological support to employees who may “want to talk to someone” from outside work but not to employees with diagnosable psychological difficulties or mental health conditions. We made further references to this issue in our previous article on triage.
Employment lawyers
One of the keys to the successful handling of a mental health issue with an employee is early intervention. Employment lawyers often see the problems that arise when the employee’s manager puts his or her head in the sand and indulges in wishful thinking that the problem will solve itself.
The notion that this sort of “problem” will go away and sort itself out by itself of course rarely happens. If, instead, the issue is picked up and addressed early the impact on everyone involved should be lessened and a positive outcome is more likely.
Having a fully developed plan, policy and support structure in place for both the sufferer and HR/management will put an [1]organisation ahead of many in the marketplace.
Legal advice needs to be tailored to ensure that the employer is fulfilling its legal duties in its response to the situation and appropriately discharging its duty of care. An employer needs to look through a different lens at problems that have a mental health angle.
Tackling these as a dispute or a battle to be won (as is often the case where an employee situation requires legal advice) is inappropriate. Instead, in our experience, the most constructive approach is to focus on the human angle both in terms of the employee with the health problem and the managers who are responsible for the employee and engaged in the situation.
If things develop such that the employee leaves the business, legal advice will address how to manage this sensitively and how to avoid/reduce risks of claims for disability discrimination, personal injury, failure of duty of care or unfair dismissal.
As every individual is different, and mental health issues can take an uncertain path, there will be no “one size fits all” approach.
It will often be the case that early intervention enables an employee to keep working and continue to be a productive member of the team. However, there will be situations where the employee is not fit for work and a period of absence or indeed an exit from the business may be the best solution.
By working with the employee to support them in times of poor mental ill health, an amicable departure should be possible. An employer should no longer find itself paying out vast sums in settlement as it will have discharged its legal obligations towards the employee.
Mental health responder (MHR) training
The organisation’s “ear to the ground” in the context of mental health are its mental health responders (MHR). MHRs receive training on mental health and wellbeing issues and are the first point of call for staff presenting with psychological or mental health problems.
The MHR’s role is to advocate with management and colleagues for measures that foster wellbeing and good mental health. They should also act as the first line of response when individuals fall through the safety net, both by reaching out to them and considering what more could be done to improve mental-health in future.
The MHR training differs from the Mental Health First Aid (MHFA) training primarily because MHRs rely on the back-up of the mental health specialist helpline and are trained to operate at the unison with HR and specialists from the mental health service provider.
Conclusion
It will be clear from this article that, just as a building requires foundation and infrastructure that rely on each other and cannot stand in isolation, the components of an organisation’s approach to sound occupational mental health in the workplace have to be interconnected, well-coordinated and able to operate as a coherent whole.
We argue that the first step towards getting your house in order is a good structural survey to ensure foundation and infrastructure.
Senior management should take action if there are any missing components as the framework’s interrelated parts need to be in place to set the organisation on a secure footing regarding mental health and wellbeing in the workplace.
Reference
Triage: the (mostly) missing link in OH mental health, Occupational Health & Wellbeing, October, 2019 (vol 70 no 10), published online on 7 December 2018, https://www.personneltoday.com/hr/triage-the-mostly-missing-link-in-oh-mental-health/
Sign up to our weekly round-up of HR news and guidance
Receive the Personnel Today Direct e-newsletter every Wednesday